A TB scientific section working group
Globally, people deprived of liberty (PDL) have extremely high rates of tuberculosis, often more than 10 times greater than the general population.1,2 Overcrowding, poor ventilation, limited access to healthcare resources, substance abuse and undernutrition are all risk factors that disproportionately affect PDL.3–6 At the same time, this population remains frequently neglected by Ministries of Health and Justice and in global TB prevention and care strategies. There is a critical need to increase attention and resources towards addressing the crisis of tuberculosis among PDL.7
The TB in Prisons Working Group seeks to engage practitioners, researchers, policy makers and advocates in raising awareness about tuberculosis among PDL and identifying and sharing best practices and guidance to improve care and prevention of TB in prisons. The Working Group will engage Union members in structured interactions to share experience and expertise on tuberculosis in prisons, to identify knowledge gaps and key areas for research, to build collaborations and consortia for research and implementation, and to create literature including reviews, perspectives, best practices documents and implementation guidance for areas where WHO guidelines are lacking. A major overarching goal of this Working Group will be to build a community of researchers and practitioners engaged in TB care and prevention in prisons to facilitate knowledge exchange and organize more effective, collaborative research and advocacy.
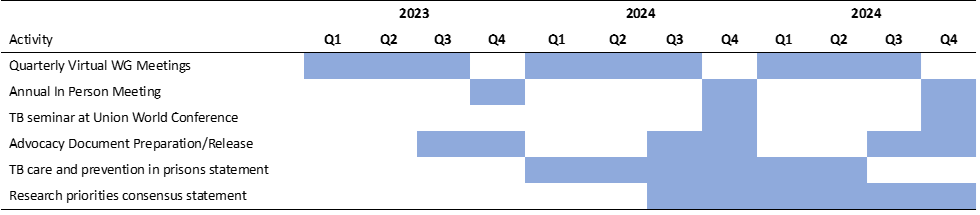
Objectives, by year:
2023: Hold a series of virtual meetings with rotating presenters on key themes in tuberculosis in prisons; hold in person meeting at Union World TB Conference
2024: Produce and distribute advocacy materials; continue regular virtual Working Group meetings; hold TB seminar and in person meeting at Union World TB conference;
2025: Finalize and distribute consensus statements on research priorities and TB care and prevention approaches in prisons; hold TB seminar and in person meeting at Union World TB conference
Activities:
- Establish a collaborative working group
- Hold a series of virtual meetings with rotating presenters from the working to share about their work and challenges of TB care and prevention in prisons in their country/community.
- Invite leaders from Ministries of Health and Justice to meetings to share experiences about TB care and prevention in prisons and learn from others about challenges and effective strategies for improvement.
- Hold an annual working group meeting at the Union World TB conference
- Propose a TB in prisons seminar, with talks by various working group members and experts, at the Union World TB conference
- Develop an advocacy strategy to improve care and prevention of TB in prisons
- The working group will schedule meetings with TB and criminal justice advocates and policy experts to learn about effective advocacy for TB in prisons.
- The working group will develop a strategy for focusing awareness and advocacy efforts, identifying key stakeholders to engage for policy advocacy.
- The working group will produce advocacy materials (e.g. fact sheets, images, etc), translated into languages spoken in high TB burden countries, to distribute to stakeholders and via social media
- Produce consensus recommendations for TB care and prevention in prisons
- There remains a lack of specific international guidance on several key issues pertaining to TB in prisons, for example: 1) specific screening strategies; 2) use of preventive therapy; 3) transitional care at release.
- For topics in which there are evidence and/or successful experiences among the working group, we will write guidance and best practices documents. We will publish these as Viewpoint or Perspective pieces and create summaries that can be used to inform country-level TB strategies.
- We will seek meetings with key stakeholders including regional (WHO regional offices / PAHO) and national (Ministries of Health) leaders to share these documents and advocate for increased investments in care and prevention in prisons
- Identify key research priorities for TB in prisons
- The working group will identify and prioritize key scientific questions that need to be answered to improve TB prevention and care in prisons.
- These knowledge gaps and research questions will be summarized in a consensus statement and shared publicly to stimulate research
- We will encourage working group members to form research consortia and apply for join funding to do multicountry studies focused on TB care and prevention in prisons.
- We will also engage with modelers (TB Modelling and Analysis Consortium) and other researchers and funders to stimulate interest in TB research in prisons.
We will invite working group members to participate in all of the activities above, including giving presentations virtually and at Union meetings, writing or providing feedback on advocacy documents, fact sheets and consensus statements, and participating in meetings with stakeholders. We will also seek to engage practitioners, clinicians, researchers and implementers who are not currently part of the Union to join the Union and play a role in the Working Group.
End deliverables:
- December, 2023 – Hold at least three virtual meetings and an in person meeting at Union World Conference to shape detailed agenda for the Working Group
- March, 2024 - Complete fact sheet and advocacy materials, distribute on World TB Day
- December, 2024 – Seminar and annual meeting at Union World Conference; Release advocacy strategy and updated materials
- December, 2025 – Release consensus paper on research priorities; consensus paper on TB care and prevention in prisons; Seminar and annual meeting at Union World Conference
Time frame & proposed date of completion:
References:
1. Cords O, Martinez L, Warren JL, O’Marr JM, Walter KS, Cohen T, Zheng J, Ko AI, Croda J, Andrews JR. Incidence and prevalence of tuberculosis in incarcerated populations: a systematic review and meta-analysis. Lancet Public Health. 2021;6(5):e300-e308. doi:10.1016/S2468-2667(21)00025-6
2. Baussano I, Williams BG, Nunn P, Beggiato M, Fedeli U, Scano F. Tuberculosis Incidence in Prisons: A Systematic Review. PLoS Med. 2010;7(12):e1000381. doi:10.1371/journal.pmed.1000381
3. Dara M, Chorgoliani D, de Colombani P. TB Prevention and Control Care in Prisons. World Health Organization - Regional Office, Europe https://www.euro.who.int/en/publications/abstracts/prisons-and-health/report-by-chapters/chapter-8.-tb-prevention-and-control-care-in-prisons
4. Hatwiinda S, Topp SM, Siyambango M, Harris JB, Maggard KR, Chileshe C, Kapata N, Reid SE, Henostroza G. Poor continuity of care for TB diagnosis and treatment in Zambian Prisons: a situation analysis. Trop Med Int Health. 2018;23(2):243-250. doi:10.1111/tmi.13024
5. Pelissari DM, Saita NM, Monroe AA, Diaz-Quijano FA. Environmental factors associated with the time to tuberculosis diagnosis in prisoners in São Paulo, Brazil. Am J Infect Control. Published online May 27, 2022:S0196-6553(22)00441-2. doi:10.1016/j.ajic.2022.05.015
6. Henostroza G, Topp SM, Hatwiinda S, Maggard KR, Phiri W, Harris JB, Krüüner A, Kapata N, Ayles H, Chileshe C, Reid SE. The high burden of tuberculosis (TB) and human immunodeficiency virus (HIV) in a large Zambian prison: a public health alert. PLoS One. 2013;8(8):e67338. doi:10.1371/journal.pone.0067338
7. Walter KS, Martinez L, Arakaki-Sanchez D, Sequera VG, Estigarribia Sanabria G, Cohen T, Ko AI, García-Basteiro AL, Rueda ZV, López-Olarte RA, Espinal MA, Croda J, Andrews JR. The escalating tuberculosis crisis in central and South American prisons. Lancet. 2021;397(10284):1591-1596. doi:10.1016/S0140-6736(20)32578-